
Laser Therapy
What is Laser Therapy?
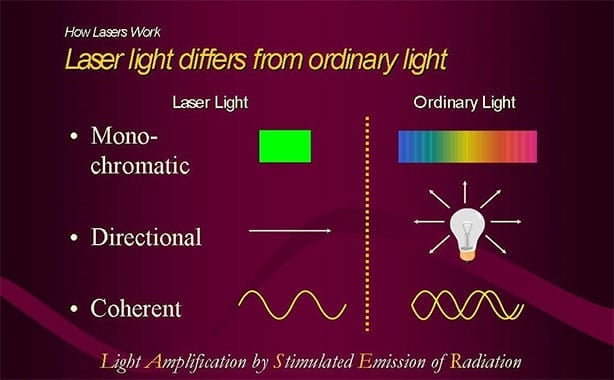
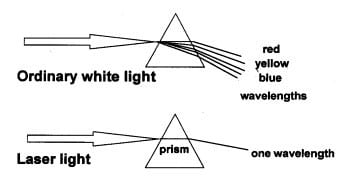
All light is composed of photons: small packets of light energy in the form of waves with a defined frequency and wavelength. However, not all light is the same. Different wavelengths of light represent different colors on the light spectrum.
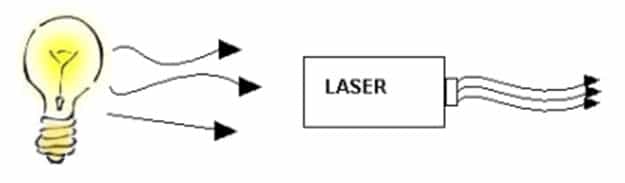
When light is projected as a single, coherent wavelength where the waves travel parallel to each other, it’s considered laser light. Laser light is much more intense than regular white light and has a multitude of applications from scanning barcodes to treating pain, inflammation, and more within human (and animal) bodies.
Laser light holds its intensity until it is absorbed by a medium; in the case of laser therapy, the medium is the body. The photon energy of laser light can effectively penetrate the skin and underlying structures, which accelerates the body’s natural healing process. Laser therapy utilizes the wavelengths and frequencies of visible red and near infrared (NIR) light to treat a variety of conditions at their source within the body through safe, non-invasive, and painless procedures.
How Laser Therapy Works
Photochemical Action
Studies have shown that when tissue cultures are irradiated by lasers, enzymes within cells absorb energy from laser light. Visible red light and near infrared (NIR) are absorbed within the mitochondria and the cell membrane. This produces higher ATP levels and boosts DNA production, leading to an increase in cellular health and energy.
Therefore, when applied as treatment, lasers have been shown to reduce pain and inflammation as well as stimulate nerve regeneration, muscle relaxation, and immune system response. Lasers have no effect on normal tissues because photons of light are only absorbed and utilized by the cells that need them.


Role of Chromophores
Chromophores are components of various cells and subcellular organelles which absorb light. The stimulation of chromophores on mitochondrial membranes incites the production of ATP. This results in:
- Increased cellular energy levels
- Pain relief
- Accelerated cellular healing
Biological Effects of Laser Therapy
Laser therapy has an antiedemic effect as it causes vasodilation (the dilation of blood vessels, decreasing blood pressure), but also because it activates the lymphatic drainage system (drains swollen areas). As a result, there is a reduction in swelling caused by bruising or inflammation.
Laser therapy has a high beneficial effect on nerve cells which block pain transmitted by these cells to the brain and which decreases nerve sensitivity. Also, due to less inflammation, there is less edema and less pain. Another pain blocking mechanism involves the production of high levels of pain killing chemicals such as endorphins and enkephalins from the brain and adrenal gland.
Photons of light from lasers penetrate deep into tissue and accelerate cellular reproduction and growth. The laser light increases the energy available to the cell so that the cell can take on nutrients faster and get rid of waste products. As a result of exposure to laser light, the cells of tendons, ligaments, and muscles are repaired faster.
Laser light will significantly increase the formation of new capillaries in damaged tissue that speeds up the healing process, closes wounds quickly and reduces scar tissue. Additional benefits include acceleration of angiogenesis, which causes temporary vasodilatation, an increase in the diameter of blood vessels.
Laser therapy creates higher outputs of specific enzymes, greater oxygen, and food particle loads for blood cells.
Laser therapy stimulates muscle trigger points and acupuncture points on a non-invasive basis, providing musculoskeletal pain relief.
Laser therapy reduces the formation of scar tissue following tissue damage from cuts, scratches, burns, or surgery.
Slow recovery of nerve functions in damaged tissue can result in numbness and impaired limbs. Laser light speeds up the process of nerve-cell reconnection and increases the amplitude of action potentials to optimize muscle action.
Laser light has a direct effect on immunity status by stimulating immunoglobulins and lymphocytes. Laser therapy is absorbed by chromophones (molecule enzymes) that react to laser light. The enzyme flavin mononucleotide is activated and starts the production of ATP (adenosine triphosphate), which is the major carrier of cell energy and the energy source for all chemical reactions in the cells.
Laser light stimulates fibroblast development in damaged tissues. Fibroblasts are the building blocks of collagen, which is predominant in wound healing. Collagen is the essential protein required to replace old tissue or to repair tissue injuries. As a result, laser therapy is effective on open wounds and burns.
History of Lasers
Light has been recognized as a source of energy and healing since the early days of recorded time. Ancient Greeks, Romans, and Egyptians practiced heliotherapy, or healing by sunlight to treat various ailments. In the 17th century, Sir Isaac Newton identified the visible spectrum of light when he separated light with a prism.
Albert Einstein first explained the theory of stimulated emission in 1917, which became the basis of laser. He hypothesized that, when the population inversion exists between upper and lower levels among atomic systems, it is possible to realize amplified stimulated emission and the stimulated emission has the same frequency and phase as the incident radiation.
However, it wasn’t until the late 1940s and ‘50s that scientists and engineers did extensive work to realize a practical device based on the principle of stimulated emission. Initially, scientists and engineers were working towards the realization of a MASER (Microwave Amplification by the Stimulated Emission of Radiation), a device that amplified microwaves for its immediate application in microwave communication systems.
The first laser was invented in 1960 by Theodore Maiman, who used ruby as a lasing medium that was stimulated using high energy flashes of intense light.
Hungarian physician, Endre Mester, was a pioneer of laser medicine, including the use of low-level laser therapy (LLLT). In 1967, only a few years after the first working laser was invented, he started his experiments with the effects of lasers on skin cancer. He is credited as the discoverer of positive biological effects of low power lasers.
By the end of the 1960’s, Mester was reporting an improved healing of wounds through low-level laser radiation. Since then, scientists and doctors have understood more about the nature of light and its positive effects on the body, developing new techniques and devices for use in medicine.
Classification of Lasers
Classification of Laser Types in the United States and Europe
Since the early 1970s, lasers have been categorized in four classes with two subclasses based on a laser’s wavelength and maximum output of power. The classes group lasers according to their ability to produce damage in exposed people, from class 1 (no hazard during normal use) to class 4 (severe hazard for eyes and skin).
| United States | Europe | |
| Class | I (1) |
1, 1M |
| II, IIa (2, 2a) | 2, 2M | |
| IIIa, IIIb (3a, 3b) | 3R, 3B | |
| IV (4) | 4 |
Laser Standards and Recommendations
The Center for Devices and Radiological Health (CDRH) is a regulatory bureau within the U.S. Federal Food and Drug Administration (FDA) of the Department of Health and Human Services. The CDRH is responsible for implementing and enforcing the laws and regulations which apply to radiation and the production of electronic products and medical devices.
Medical devices, including laser therapy systems, require clearance by the FDA in order to be introduced commercially in the United States. The clearance can follow the review of a premarket notification under section 510(k) of the Federal Food, Drug, and Cosmetic Act (FFDCA) for a device that is substantially equivalent to a device that was in commercial distribution in the United States prior to May 1976 or to previously cleared devices. Clearances are device-specific and for indications claimed in the cleared labeling.
- CDRH: The Center for Devices and Radiological Health
- IEC: The International Electrotechnical Commission
ANSI: The American National Standards Institute
Some states currently require registration of medical lasers. The regulations cover use of class IIIB and IV medical lasers and require following specific guidelines for use.

Maximum Permissible Exposure (MPE)
MPE is the maximum level of laser radiation to which a person may be exposed without hazardous effects or biological changes in the eye or skin. The MPE is determined by the wavelength of a laser, the energy involved, and the duration of the exposure. MPE is a necessary in determining appropriate optical density and the nominal hazard zone.
Overview of Laser Classification
The Food and Drug Administration (FDA) recognizes four major hazard classes (I to IV) of lasers, including three subclasses (IIa, IIIa, and IIIb). The higher the class, the more powerful the laser and the potential to pose serious danger if used improperly. The labeling for Classes II–IV must include a warning symbol that states the class and the output power of the product. International Electrotechnical Commission (IEC) equivalent classes are included for products labeled under the classification system of the IEC.
The CDRH has been chartered by Congress to standardize the performance safety of manufactured laser products. The potential risks by laser class and examples of these lasers are listed in the chart below:
Potential Hazards of Laser Classes with Product Examples
| Class: FDA | Class: IEC | Laser Product Hazard | Product Examples |
| I | 1, 1M | Considered non-hazardous. Hazard increases if viewed with optical aids, including magnifiers, binoculars, or telescopes. | Laser printers, CD/DVD players |
| II, IIa | 2, 2M | Hazard increases when viewed directly for long periods of time. Hazard increases if viewed with optical aids. | Barcode scanners |
| IIIa | 3R | Depending on power and beam area, can be momentarily hazardous when directly viewed or when staring directly at the beam with an unaided eye. Risk of injury increases when viewed with optical aids. | Laser pointers |
| IIIb | 3B | Immediate skin hazard from direct beam and immediate eye hazard when viewed directly. | Laser light show projectors, industrial lasers, research lasers |
| IV | 4 | Immediate skin hazard or eye hazard from exposure to either the direct or reflected beam; may also present a fire hazard. | Laser light show projectors, industrial lasers, research lasers, lasers used to perform LASIK eye surgery. |
Class III vs Class IV Laser Therapy

The authors of Laser Therapy – Clinical Practice and Scientific Background, Dr. Jan Tuner and Lars Hode, have performed an analysis of a number of frequently cited studies on the effects of low level laser therapy (LLLT). Selected Quotes:
- “In many of these studies, analysis uncovered one or more reasons for the negative findings reported, the most common being the use of extremely low doses.”
- “The trend in laser therapy for the past 10 years has been to increase power density and dose, since this has been shown to improve therapeutic outcomes considerably.”
- “There is no point in increasing the dose if the wavelength has a low penetration factor; the penetration of the particular wavelength must be taken into account.”
- “For the moment, we must rely on our own clinical experience. That experience, however, is so encouraging that it cannot be ignored, even with lack of scientific support. It would appear that “high powered” therapeutic lasers will be able to further expand the scope of laser therapy.”
- “I can see two alternatives for myself: to speak up and start a conflict within the laser community, maybe discrediting the therapy itself in the eyes of the general public or to keep quiet and let US practitioners pay a lot of money for very low-powered lasers, leaving us with dissatisfied customers and discredit from those who are supposed to use laser therapy in medicine.”
Class III Therapy Lasers Are Not Effective
“While the FDA has approved the marketing of the device, many payers have declined to recognize LLLT as effective treatment. Results of treatment have not been consistent so that it is difficult to state that such treatment would be necessary. Last, given the reported number of visits required to be nine to 12 visits, the cost of such treatment would be approximately $1000 to $1500. These costs appear to be somewhat unreasonable for a treatment that has not been demonstrated in the medical literature to be effective.”
Source: Position Paper on Low Level Laser Therapy (LLLT), Ohio Bureau of Workers’ Compensation
“Aetna considers cold laser therapy experimental and investigational because there is inadequate evidence of the effectiveness of low-energy (cold) lasers in wound healing, pain relief, or for other indications such as musculoskeletal dysfunction, arthritis, and neurological dysfunctions.”
Source: Aetna: Clinical Policy Bulletins, Number 0363, Subject: Cold Laser Therapy


Class IV Therapy Lasers: The Next Generation of Laser Therapy
The laws of laser physics have demonstrated that the higher the wavelength, the deeper the penetration. Penetration is paramount in order to stimulate deep musculoskeletal, vascular, lymphatic, and neurological structures.
If Class III lasers are therapeutically ineffective, it is because of insufficient energy or dosage, combined with poor penetration.
Characteristics of Class IV Therapy Lasers
Class IV lasers offers better therapeutic outcome, based on six characteristics of this new technology:
- Larger dosages of therapeutic energy: Class IV lasers can deliver up to 1,500 times more energy than Class III and, consequently, reduce treatment time.
- Deeper penetration into the body: Leading Class III lasers only penetrate 0.5-2.0cm2. Class IV can penetrate up to 10cm2.
- Larger treatment surface area: Class III cover a treatment area of 0.3-5.0cm2, depending on the model and manufacturer. Class IV cover up to 77cm2. This is important when treating large regions, such as the lumbar spine, quadriceps, or hips.
- Greater power density: Power density indicates the degree of concentration of the power output. This property has been shown to play a major role in therapeutic outcomes.
- Continuous power supply: In Class III lasers, the power is pulsed or modulated approximately 50% of the time. In other words, light is permitted to pass through the probe for only 50% of the total operating time. In most cases, Class IV lasers deliver a consistent amount of energy over a given time. Their power can be adjusted for acute and chronic conditions.
- Superior fiber optic cables: Fiber optic cables transmit laser energy from the laser to the treatment probe (wand) at the end of the cable. Several studies reveal that as much as 50% of the light energy generated by a Class III laser may be lost by the time it reaches the end of the probe.

Conclusion on Laser Therapy
Laser therapy has gained a lot of popularity in recent years for pain relieving and inflammation reducing treatments. Stimulation of the body’s cells by controlled laser applications promotes the natural healing processes of the body with a non-invasive, painless, and drug-free procedure.
Lasers have their foundation in stimulated emission first proposed by Albert Einstein in 1917, and they have come a long way from the first working laser built in 1960. Laser devices, including those used in medical and therapeutic applications, are regulated by several governing bodies, including an extension of the FDA, the Center for Devices and Radiological Health (CDRH) and the International Electrotechnical Commission.
Lasers are classified into four classes, with class III and class IV being those used in clinical applications. Class IV lasers can safely penetrate deeper to treat down to musculoskeletal levels within the body, and are the optimal class for therapeutic treatments.
If you’re interested in learning more about lasers and how laser therapy works, check out Aspen Laser University.
Laser Safety Training Program Now Available
We have partnered with Laser Safety Certification, Inc, a nationally recognized laser safety consulting company, to develop a new and
exclusive “3 in 1” Laser Safety Training and Certification Program.


